



 Copy to clipboard
Copy to clipboard 
Hospital supply chains have long emphasized cost management, but true transformation depends upon how effectively physicians can lead and support sustainable change in orthopedic and spine care.
A broader cultural shift in healthcare is the move from unrestricted physician choice to purchasing decisions informed by both quality and cost—and while supply chain leaders and executives are conversant about value, many physicians are still developing this fluency.
To start, shifting from physician preference products to clinically vetted alternatives is just as much about trust, credibility and culture as it is about data. This is why physician leaders are essential in modeling confidence and guiding peers through change. Without physician engagement, cost initiatives risk being dismissed as financial mandates. With leadership, value becomes a shared mission uniting clinical and administrative stakeholders.
Market Trends Redefining Orthopedics
The urgency for physician leadership is heightened by changing market dynamics such as the site-of-care shift, where cases are steadily moving from inpatient hospitals to ambulatory surgical centers (ASC). Orthopedic procedures are among the leading categories driving this transition, according to Sg2 forecasts (Figures 1 and 2).
Figures 1 and 2: Inpatient and Outpatient Orthopedic Forecasts
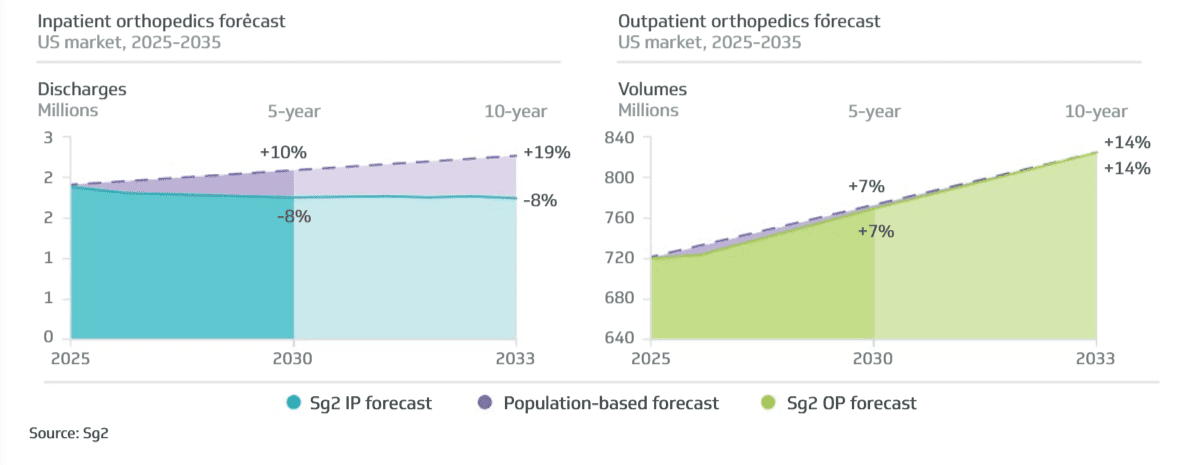
Site-of-care shifts have broad implications for health systems, including changes in reimbursement and in how patients with higher-acuity cases and more complex comorbidities are cared for in hospital settings. It also impacts the evolving dynamic between hospital leaders and surgeons, both of whom are collaborating and competing for ASC surgical cases.
Alongside those market shifts, innovations such as reverse shoulder replacements, computer-assisted navigation, and custom implants are expanding eligibility and improving outcomes. However, reimbursement for these procedures remains uncertain, especially around digital rehab and bundled payment models like the TEAM program.
The Role of Physician Leaders
As payment models evolve and outpatient growth accelerates, physician leaders will remain central to change. Their ability to navigate tension, foster trust and model value-based decision-making will be key to long-term success.
Two orthopedic surgeons and established medical leaders in Vizient’s Excelerate member systems share their insight into how governance, engagement and culture can drive system-wide value. Their viewpoints are meant to provide orthopedic companies with a glimpse into how surgeon leadership within health systems is changing, as well as how physician mindset is evolving when it comes to deciding which products to use and driving financial success within a service line.
Driving Value through Physician Leadership
Henry Boucher, M.D., Vice President of Medical Operations at MedStar Medical Group and Professor of Orthopedic Surgery at Georgetown University School of Medicine, led an effort to improve spend compliance across several service lines at MedStar Health by combining his expertise as a practicing orthopedic surgeon with his responsibilities as a system leader. The effort paid off with increased physician engagement and substantial savings.
Balancing clinical care and system leadership
Dr. Boucher oversees the neuromuscular and cardiovascular service lines while continuing to perform hip and knee replacements. In addition to his surgical and operational responsibilities, Dr. Boucher serves as MedStar’s medical director for Excelerate, overseeing category initiatives in orthopedics, cardiovascular and surgical services. He’s also a member of the Excelerate Medical Advisory Board. Each of these roles allows him to bridge clinical leadership and supply chain strategy, ensuring physician perspectives inform decision making.
MedStar Health is the largest provider in the Maryland/Washington D.C. region by patient volume. It operates 10 hospitals and multiple outpatient sites with annual revenue exceeding $8 billion. The medical staff includes both employed and private physicians practicing across academic medical centers and community hospitals. Strategic service lines include orthopedics, neurosciences, cardiovascular, oncology, GI and transplant.
Physician culture is defined by two competing realities: a strong desire for autonomy in clinical decision-making and a “One MedStar” mentality supported by governance councils. Past savings initiatives in physician preference items highlighted both the opportunities and challenges in aligning clinicians.
Common concerns at MedStar mirror those across the country: reticence to change suppliers, lack of awareness of alternate supplier portfolios, concerns about vendor service levels, belief that currently-used products are superior, and conflicts of interest.
“Not all physicians welcome change, particularly when it challenges their preferred products or long-standing vendor relationships,” Dr. Boucher said. “These concerns highlight why physician-led, credible and transparent leadership is indispensable. It’s important for physicians to be engaged early on in conversations around these products or vendors if there’s any hope of success.”
Under Dr. Boucher’s leadership, MedStar has achieved considerable progress, including the active pursuit of spend compliance across orthopedics, cardiovascular, and surgical services; substantial savings and a downward trend in price index; and improved physician engagement with system-wide sourcing initiatives.
Lessons learned
Dr. Boucher underscores that sustainable change requires both process discipline and organizational cultural sensitivity. His key lessons include:
- Engaged physician leadership is critical to credibility
- Transparent, responsive communication builds trust
- Accurate and reliable data are essential to persuading physicians
- Stakeholder inclusion should begin early and remain consistent
- Patience and empathy are needed to manage transitions
- Anticipating vendor reactions to consolidation reduces disruption
- Minimizing barriers to product evaluation and training speeds adoption
Looking ahead
As organizations look to develop physician leadership and governance structures, Dr. Boucher emphasizes three essential starting points.
First, identify a credible, visible physician champion. Early leadership must come from someone who has the trust of peers and the respect of hospital leadership. Second, build a collaborative supply chain and operations team. Success requires senior staff with authority to make decisions and align with physicians. Third, secure visible support from system leadership. Engagement from the C-suite shows commitment and provides the necessary organizational backing.
Dr. Boucher frames the shift toward value-based care as both a necessity and an opportunity. Rising financial pressures demand novel approaches, but sustainable change will only occur when physicians themselves own the process.
The central issue for MedStar—and for systems nationwide—is how quickly physicians can move from individual preference to shared accountability for cost and quality.
Physician Leadership, Financial Strategy and the Future of Orthopedics
For James Lebolt, DO, MBA, Orthopedic Surgeon, Orthopedic Sports Medicine, Division Chief, Orthopedic Surgery, Corewell Health West, leadership in healthcare has never been about titles alone—it’s about credibility, trust and translating clinical experience into strategic impact.
Early in his career, he recognized a common misconception in medicine: Busy clinicians automatically make good leaders. Clinical excellence, he argues, is important but not enough. Leadership requires intentional development, perspective and a willingness to engage in broader organizational priorities.
“I’ve always loved clinical practice, but my aspiration was also to have a seat at the table,” Dr. Lebolt said. “I wanted to participate in strategy, decision-making and business planning while maintaining the trust and credibility that comes from walking the same path as my peers.”
Dr. Lebolt defines the essence of effective physician leadership as:
- Credibility rooted in shared clinical experience
- Representation of peers rather than authority over them
- Active listening, recognizing that physicians often want to be heard more than directed
- Applying diagnostic reasoning from clinical training to organizational problem-solving
- Helping physicians shift from an individual mindset to one of team-based, value-aligned success
He also believes surgeons’ natural competitiveness, when channeled toward system goals, can drive innovation and accelerate cultural change.
A translational role: Bridging physicians and systems
In his current leadership role, Dr. Lebolt describes himself as a translator between health systems and medical staff. His goal is to help each group understand the other’s language, pressures and priorities, thereby reducing tension and strengthening collaboration.
He points to a cultural shift underway: Moving from a “hospital vs. physician” dynamic toward a collaborative “surgeon/system/vendor” mindset. When physicians and systems align, they can work together to balance clinical quality, financial sustainability and vendor relationships.
“Smart physicians are increasingly making value-driven decisions,” he said. “The key is transparency, especially with financial data. When you give physicians a clear line of sight into cost and performance, they respond thoughtfully.”
Achievements under Dr. Lebolt’s leadership projects thus far have included completing an endomechanical conversion; executing a hip and knee implant agreement, with implementation currently underway; undergoing a year-long trial with urinary catheters in a large, system-wide conversion; removing trauma products and non-awarded suppliers in a phased approach with collaboration from surgeon stakeholders.
Lessons learned
One of Dr. Lebolt’s most consistent practices is the routine sharing of financial data with physicians. By anchoring operational discussions in real-world numbers, he ensures financial implications are treated not as an afterthought but as a shared responsibility. Transparency, he stresses, is the foundation of trust and effective decision-making.
For recruitment and retention, he emphasizes that medical staff should hire for value and present a proposition that resonates with both mission and margin. What physicians value often reflects where they are in their careers: Early-career physicians often embrace innovation and flexibility, mid-career physicians balance value with efficiency and outcomes, and later-career physicians tend to prioritize stability and view value as part of their professional legacy.
For Dr. Lebolt, physician governance is non-negotiable. He said top-down models rarely achieve durable results, and that success comes from engaging practicing clinicians, not just administrative leaders. Additionally, collaborative structures where physicians participate in shaping policy generate better decisions and stronger adoption. Though this approach takes more time and effort, it builds an organizational culture rooted in trust, accountability and lasting engagement.
Dr. Lebolt offers practical guidance for organizations seeking to establish or strengthen governance structures.
First, healthcare systems should invest in actively practicing physician leaders. These leaders bring immediate credibility because they share the same challenges as their peers. While reducing clinical time may decrease short-term volume, their involvement ensures better alignment and helps frame difficult decisions as opportunities for mutual benefit.
Second, providers should offer meaningful education and development resources. Equip physician leaders with training in organizational and industry challenges—through MBA programs, peer networks like the American Association for Physician Leadership or leadership forums such as the Health Management Academy. Ongoing development allows leaders to translate between system priorities and physician needs effectively.
Looking ahead
Dr. Lebolt anticipates significant shifts in orthopedic care delivery driven by workforce shortages and technology adoption. According to projections from the Health Resources and Services Administration, the U.S. currently faces a shortage of more than 5,000 orthopedic surgeons. Health systems must prepare now to ensure future access and efficiency in patient care.
Dr. Lebolt’s leadership philosophy is both pragmatic and aspirational; it’s grounded in credibility, informed by data and centered on cultural alignment. His approach reflects the evolving expectations of orthopedic surgeons today, where collaboration, transparency and vision are as essential as clinical skill. As health systems grapple with financial pressure, workforce shortages and shifting models of care, leaders like Dr.
Lebolt demonstrate that the future of orthopedics will be defined not only by surgical innovation, but by physician leadership that bridges mission and margin.
Conclusion
Change in orthopedics inevitably creates tension, particularly when long-standing habits and product loyalties are challenged. Effective physician leaders view this tension not as an obstacle, but as a natural by-product of meaningful transformation.
By embracing dialogue, modeling transparency and engaging peers constructively, leaders can address concerns while guiding teams through change. As Drs. Boucher and Lebolt emphasize, physician leaders must “walk the walk,” communicate openly and involve colleagues early and throughout planning, implementation and measurement.
Physician leaders are the driving force behind sustainable, value-based change in orthopedics and spine. Their credibility, transparency and cultural influence determine how well health systems adapt in an era of cost pressure and innovation. Health systems that invest in and empower physician leadership and orthopedic companies that build strategies that help further this dynamic will be best positioned to thrive.
A version of this article was originally published by Vizient in Medical Device Tech Watch and is reprinted with permission.
Hospital supply chains have long emphasized cost management, but true transformation depends upon how effectively physicians can lead and support sustainable change in orthopedic and spine care.
A broader cultural shift in healthcare is the move from unrestricted physician choice to purchasing decisions informed by both quality and cost—and...
Hospital supply chains have long emphasized cost management, but true transformation depends upon how effectively physicians can lead and support sustainable change in orthopedic and spine care.
A broader cultural shift in healthcare is the move from unrestricted physician choice to purchasing decisions informed by both quality and cost—and while supply chain leaders and executives are conversant about value, many physicians are still developing this fluency.
To start, shifting from physician preference products to clinically vetted alternatives is just as much about trust, credibility and culture as it is about data. This is why physician leaders are essential in modeling confidence and guiding peers through change. Without physician engagement, cost initiatives risk being dismissed as financial mandates. With leadership, value becomes a shared mission uniting clinical and administrative stakeholders.
Market Trends Redefining Orthopedics
The urgency for physician leadership is heightened by changing market dynamics such as the site-of-care shift, where cases are steadily moving from inpatient hospitals to ambulatory surgical centers (ASC). Orthopedic procedures are among the leading categories driving this transition, according to Sg2 forecasts (Figures 1 and 2).
Figures 1 and 2: Inpatient and Outpatient Orthopedic Forecasts
Site-of-care shifts have broad implications for health systems, including changes in reimbursement and in how patients with higher-acuity cases and more complex comorbidities are cared for in hospital settings. It also impacts the evolving dynamic between hospital leaders and surgeons, both of whom are collaborating and competing for ASC surgical cases.
Alongside those market shifts, innovations such as reverse shoulder replacements, computer-assisted navigation, and custom implants are expanding eligibility and improving outcomes. However, reimbursement for these procedures remains uncertain, especially around digital rehab and bundled payment models like the TEAM program.
The Role of Physician Leaders
As payment models evolve and outpatient growth accelerates, physician leaders will remain central to change. Their ability to navigate tension, foster trust and model value-based decision-making will be key to long-term success.
Two orthopedic surgeons and established medical leaders in Vizient’s Excelerate member systems share their insight into how governance, engagement and culture can drive system-wide value. Their viewpoints are meant to provide orthopedic companies with a glimpse into how surgeon leadership within health systems is changing, as well as how physician mindset is evolving when it comes to deciding which products to use and driving financial success within a service line.
Driving Value through Physician Leadership
Henry Boucher, M.D., Vice President of Medical Operations at MedStar Medical Group and Professor of Orthopedic Surgery at Georgetown University School of Medicine, led an effort to improve spend compliance across several service lines at MedStar Health by combining his expertise as a practicing orthopedic surgeon with his responsibilities as a system leader. The effort paid off with increased physician engagement and substantial savings.
Balancing clinical care and system leadership
Dr. Boucher oversees the neuromuscular and cardiovascular service lines while continuing to perform hip and knee replacements. In addition to his surgical and operational responsibilities, Dr. Boucher serves as MedStar’s medical director for Excelerate, overseeing category initiatives in orthopedics, cardiovascular and surgical services. He’s also a member of the Excelerate Medical Advisory Board. Each of these roles allows him to bridge clinical leadership and supply chain strategy, ensuring physician perspectives inform decision making.
MedStar Health is the largest provider in the Maryland/Washington D.C. region by patient volume. It operates 10 hospitals and multiple outpatient sites with annual revenue exceeding $8 billion. The medical staff includes both employed and private physicians practicing across academic medical centers and community hospitals. Strategic service lines include orthopedics, neurosciences, cardiovascular, oncology, GI and transplant.
Physician culture is defined by two competing realities: a strong desire for autonomy in clinical decision-making and a “One MedStar” mentality supported by governance councils. Past savings initiatives in physician preference items highlighted both the opportunities and challenges in aligning clinicians.
Common concerns at MedStar mirror those across the country: reticence to change suppliers, lack of awareness of alternate supplier portfolios, concerns about vendor service levels, belief that currently-used products are superior, and conflicts of interest.
“Not all physicians welcome change, particularly when it challenges their preferred products or long-standing vendor relationships,” Dr. Boucher said. “These concerns highlight why physician-led, credible and transparent leadership is indispensable. It’s important for physicians to be engaged early on in conversations around these products or vendors if there’s any hope of success.”
Under Dr. Boucher’s leadership, MedStar has achieved considerable progress, including the active pursuit of spend compliance across orthopedics, cardiovascular, and surgical services; substantial savings and a downward trend in price index; and improved physician engagement with system-wide sourcing initiatives.
Lessons learned
Dr. Boucher underscores that sustainable change requires both process discipline and organizational cultural sensitivity. His key lessons include:
- Engaged physician leadership is critical to credibility
- Transparent, responsive communication builds trust
- Accurate and reliable data are essential to persuading physicians
- Stakeholder inclusion should begin early and remain consistent
- Patience and empathy are needed to manage transitions
- Anticipating vendor reactions to consolidation reduces disruption
- Minimizing barriers to product evaluation and training speeds adoption
Looking ahead
As organizations look to develop physician leadership and governance structures, Dr. Boucher emphasizes three essential starting points.
First, identify a credible, visible physician champion. Early leadership must come from someone who has the trust of peers and the respect of hospital leadership. Second, build a collaborative supply chain and operations team. Success requires senior staff with authority to make decisions and align with physicians. Third, secure visible support from system leadership. Engagement from the C-suite shows commitment and provides the necessary organizational backing.
Dr. Boucher frames the shift toward value-based care as both a necessity and an opportunity. Rising financial pressures demand novel approaches, but sustainable change will only occur when physicians themselves own the process.
The central issue for MedStar—and for systems nationwide—is how quickly physicians can move from individual preference to shared accountability for cost and quality.
Physician Leadership, Financial Strategy and the Future of Orthopedics
For James Lebolt, DO, MBA, Orthopedic Surgeon, Orthopedic Sports Medicine, Division Chief, Orthopedic Surgery, Corewell Health West, leadership in healthcare has never been about titles alone—it’s about credibility, trust and translating clinical experience into strategic impact.
Early in his career, he recognized a common misconception in medicine: Busy clinicians automatically make good leaders. Clinical excellence, he argues, is important but not enough. Leadership requires intentional development, perspective and a willingness to engage in broader organizational priorities.
“I’ve always loved clinical practice, but my aspiration was also to have a seat at the table,” Dr. Lebolt said. “I wanted to participate in strategy, decision-making and business planning while maintaining the trust and credibility that comes from walking the same path as my peers.”
Dr. Lebolt defines the essence of effective physician leadership as:
- Credibility rooted in shared clinical experience
- Representation of peers rather than authority over them
- Active listening, recognizing that physicians often want to be heard more than directed
- Applying diagnostic reasoning from clinical training to organizational problem-solving
- Helping physicians shift from an individual mindset to one of team-based, value-aligned success
He also believes surgeons’ natural competitiveness, when channeled toward system goals, can drive innovation and accelerate cultural change.
A translational role: Bridging physicians and systems
In his current leadership role, Dr. Lebolt describes himself as a translator between health systems and medical staff. His goal is to help each group understand the other’s language, pressures and priorities, thereby reducing tension and strengthening collaboration.
He points to a cultural shift underway: Moving from a “hospital vs. physician” dynamic toward a collaborative “surgeon/system/vendor” mindset. When physicians and systems align, they can work together to balance clinical quality, financial sustainability and vendor relationships.
“Smart physicians are increasingly making value-driven decisions,” he said. “The key is transparency, especially with financial data. When you give physicians a clear line of sight into cost and performance, they respond thoughtfully.”
Achievements under Dr. Lebolt’s leadership projects thus far have included completing an endomechanical conversion; executing a hip and knee implant agreement, with implementation currently underway; undergoing a year-long trial with urinary catheters in a large, system-wide conversion; removing trauma products and non-awarded suppliers in a phased approach with collaboration from surgeon stakeholders.
Lessons learned
One of Dr. Lebolt’s most consistent practices is the routine sharing of financial data with physicians. By anchoring operational discussions in real-world numbers, he ensures financial implications are treated not as an afterthought but as a shared responsibility. Transparency, he stresses, is the foundation of trust and effective decision-making.
For recruitment and retention, he emphasizes that medical staff should hire for value and present a proposition that resonates with both mission and margin. What physicians value often reflects where they are in their careers: Early-career physicians often embrace innovation and flexibility, mid-career physicians balance value with efficiency and outcomes, and later-career physicians tend to prioritize stability and view value as part of their professional legacy.
For Dr. Lebolt, physician governance is non-negotiable. He said top-down models rarely achieve durable results, and that success comes from engaging practicing clinicians, not just administrative leaders. Additionally, collaborative structures where physicians participate in shaping policy generate better decisions and stronger adoption. Though this approach takes more time and effort, it builds an organizational culture rooted in trust, accountability and lasting engagement.
Dr. Lebolt offers practical guidance for organizations seeking to establish or strengthen governance structures.
First, healthcare systems should invest in actively practicing physician leaders. These leaders bring immediate credibility because they share the same challenges as their peers. While reducing clinical time may decrease short-term volume, their involvement ensures better alignment and helps frame difficult decisions as opportunities for mutual benefit.
Second, providers should offer meaningful education and development resources. Equip physician leaders with training in organizational and industry challenges—through MBA programs, peer networks like the American Association for Physician Leadership or leadership forums such as the Health Management Academy. Ongoing development allows leaders to translate between system priorities and physician needs effectively.
Looking ahead
Dr. Lebolt anticipates significant shifts in orthopedic care delivery driven by workforce shortages and technology adoption. According to projections from the Health Resources and Services Administration, the U.S. currently faces a shortage of more than 5,000 orthopedic surgeons. Health systems must prepare now to ensure future access and efficiency in patient care.
Dr. Lebolt’s leadership philosophy is both pragmatic and aspirational; it’s grounded in credibility, informed by data and centered on cultural alignment. His approach reflects the evolving expectations of orthopedic surgeons today, where collaboration, transparency and vision are as essential as clinical skill. As health systems grapple with financial pressure, workforce shortages and shifting models of care, leaders like Dr.
Lebolt demonstrate that the future of orthopedics will be defined not only by surgical innovation, but by physician leadership that bridges mission and margin.
Conclusion
Change in orthopedics inevitably creates tension, particularly when long-standing habits and product loyalties are challenged. Effective physician leaders view this tension not as an obstacle, but as a natural by-product of meaningful transformation.
By embracing dialogue, modeling transparency and engaging peers constructively, leaders can address concerns while guiding teams through change. As Drs. Boucher and Lebolt emphasize, physician leaders must “walk the walk,” communicate openly and involve colleagues early and throughout planning, implementation and measurement.
Physician leaders are the driving force behind sustainable, value-based change in orthopedics and spine. Their credibility, transparency and cultural influence determine how well health systems adapt in an era of cost pressure and innovation. Health systems that invest in and empower physician leadership and orthopedic companies that build strategies that help further this dynamic will be best positioned to thrive.
A version of this article was originally published by Vizient in Medical Device Tech Watch and is reprinted with permission.

You’ve reached your limit.
We’re glad you’re finding value in our content — and we’d love for you to keep going.
Subscribe now for unlimited access to orthopedic business intelligence.

PV
Patrick Vega is Consulting Director for Vizient’s Excelerate and PPI Orthopedics. Mr. Vega consults to member hospitals, health systems and physicians in musculoskeletal services with a focus on high-value care by aligning cost, quality and performance.





